-
Background
A 64-year-old retired, male presented in our office with right knee pain. He described having an active lifestyle prior to the onset of the knee pain, as well as being a former member of the armed services. He previously received a diagnosis of osteoarthritis (OA) of the medial compartment from a local orthopedic clinic. Over the course of seven months, the he underwent conservative treatments including cortisone and viscosupplement injections, physical therapy and bracing with no prolonged pain relief.
-
The Case
Following the failed conservative treatments, the patient researched the surgical options to treat advanced OA of the knee. From that research, he was interested in determining if he could be a candidate for a unicompartmental (partial) knee arthroplasty, which led him to our practice.
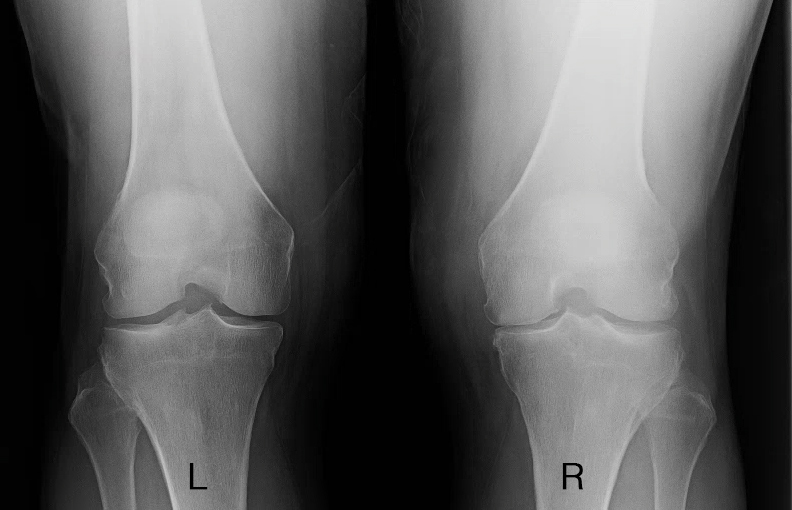
Prior to presenting in our office, the patient had obtained standing radiographs, which lead to a diagnosis of medial compartmental osteoarthritis. After examining the knee to rule out any ligamentous insufficiency, we discussed the options for arthroplasty. The patient was interested whether he was better suited for a partial or total knee arthroplasty.
Over the course of the conversation, the physician noted that a magnetic resonance imaging (MRI) study was an option for examining the extent of the patient’s osteoarthritis, but that there is a possibility of an inconclusive result in the lateral and/or patellofemoral compartments. The patient was also presented with the option of an in-office diagnostic arthroscopy via the mi-eye 2™ to examine the compartments in real-time. Due to the patient’s desire to obtain a definitive answer prior to him making a final decision on surgery, he opted for the in-office arthroscopy.

The Answer
The patient was positioned sitting upright on the office exam table with his leg suspended from the edge to create 90-degrees of initial flexion. The procedure site was prepared with a standard, sterile protocol utilizing betadine to aseptically clean the area. Local anesthesia was administered in the knee using 10cc of 1% lidocaine with epinephrine and 10cc of 0.25% marcaine in a skin wheel and a small amount was used in the capsule. An ethyl chloride topical spray was used on the knee as the local anesthesia needle was introduced. The patient was then left for eight minutes to allow the anesthesia to adequately anesthetize the joint.
The mi-eye 2™ was inserted into the anterolateral portal to assess the extent of degenerative changes to the articular cartilage. Upon examination of the patient’s lateral compartment, notable arthritic changes were visualized through the mi-eye 2™. Next, the patellofemoral compartment was examined, which also showed degenerative changes consistent with osteoarthritis. Finally, the mi-eye 2™ visualized the patient’s previously diagnosed osteoarthritis in the medial compartment. As a result of the patient’s tricompartmental OA, it was recommended that he be treated with a total knee arthroplasty (TKA). The patient was then referred to a partner in our practice that specializes in total knee arthroplasty.


Discussion
In this case, the use of the mi-eye 2™ allowed our patient to have a definitive answer regarding whether or not he was a candidate for a partial knee replacement. By performing the in-office diagnostic arthroscopy, the patient and physician were able to get a real-time look at his knee and obtain an immediate answer on the extent of the degeneration. If the patient had opted for an MRI, in place of the mi-eye 2™, it is possible that it may have been inconclusive for osteoarthritis in the lateral and patellofemoral compartments, which the mi-eye 2™ visualized.
In addition, if the treatment plan had been based solely on the patient’s previous x-ray and symptoms, he may have been a candidate for a partial knee replacement to treat the medial compartment degeneration. Had the partial replacement been performed, the patient may have developed worsening lateral pain later in life. With the diagnosis of tricompartmental OA, this patient will likely have longer lasting relief with a total knee replacement to not only treat his current knee pain now, but potentially alleviate the concern of managing additional pain later in life.