-
Background
A 38-year-old, male patient presented in office with subacute left knee pain for 2 months without prior injury. Non-steroidal anti-inflammatory drugs (NSAIDs) proved to be minimally effective in alleviating the pain. Upon physical examination the patient demonstrated minimal swelling, medial joint line pain and a negative McMurray’s test.
-
The Case
A standard of care, Magnetic Resonance Imaging (MRI), would typically be ordered, at this point, to aid in the diagnostic process of the patient’s knee pain. However, due to metal shrapnel in his flank from an improvised explosive device (IED), he was not an MRI candidate. The patient was presented with the option of an in-office diagnostic arthroscopy performed using the mi-eye 2TM and he consented to the procedure.
The Answer
The patient was positioned sitting upright on the exam room table. After cleaning the patient’s knee with ChloraPrep, the standard, subpatellar medial and lateral knee portals were anesthetized utilizing a combination of 1% lidocaine and 0.5% bupivacaine. After allowing ten minutes for the anesthetic to numb the joint, the patient was then re-positioned supine on the exam room table with his left leg positioned to the side of the table. The knee was re-prepped using ChloraPrep.
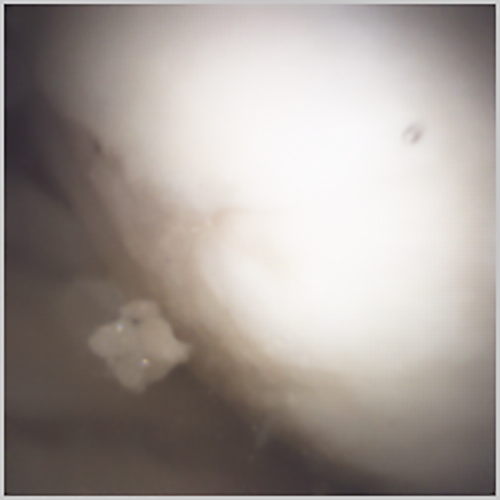
The mi-eye 2™ scope was introduced into the joint first through the lateral portal. The medial femoral condyle was observed to have a full thickness chondral defect that encompassed approx. 40% of the femoral condyle (Figure 1). The mi-eye 2™ was then placed into the medial portal and the lateral and patellofemoral compartments were examined. The mi-eye 2™ aided in the visualization of the remaining cartilage and menisci, which were normal. Due to the size of the defect and the presence of pristine adjacent cartilage, it was recommended that the patient undergo an osteochondral allograft transplant (OATS) procedure. The staged procedure was performed after fresh allograft was procured.

Discussion
In-office arthroscopy is an important procedure that can assist surgeons with diagnostic challenges such as the non-MRI candidate described in this case. Innovations in the technology of disposable cameras with small, high-resolution lens have allowed in-office arthroscopy to become a valuable tool for surgeons, patients, and insurance. The procedure has been shown to be a cost saving procedure compared to an MRI. However, in-office knee arthroscopy adds intangible advantages beyond direct costs. It also allows for real-time visualization of the intra-articular knee, more efficient diagnosis for both the patient and physician, and the ability to provide appropriate and directed injection therapies such as platelet rich plasma (PRP) or intra-articular steroids.
There are some limitations to in-office arthroscopy, including extra-articular knee injuries such as medial collateral ligament or posterolateral corner injuries, and acute hemarthrosis following a cruciate ligament tear or intra-articular fracture. Beyond these contra-indications, in-office arthroscopy is a valuable diagnostic tool for intra-articular injuries including evaluation of cartilage injuries